
Cystocele
A cystocele (also known as an anterior prolapse) is a hernia of the front vaginal wall resulting in the bladder bulging into the vaginal passage. Pelvic organ prolapse is often measured in stages ranging from stage 1 which is a minor prolapse, to stage 4 which is complete prolapse. If you are suffering from one type of pelvic organ prolapse, the pull on your organs and connective tissues can also cause other prolapses to occur. It is very important to begin pelvic floor muscle training as soon as possible to regain the strength in your pelvic floor and lessen the symptoms of your cystocele.
Because a cystocele causes the bladder to be pulled/pushed into the vagina, the urethra is often impacted. This can prevent you from starting the flow of urine when you feel the need to pee. Sometimes women with cystocele have to splint by lifting the bladder from inside the vagina in order to pee. There can also be difficulty with emptying the bladder fully which can lead to urinary tract infections (UTI). Cystocele symptoms can also have negative impact on sexual function.
Grades of Cystocele
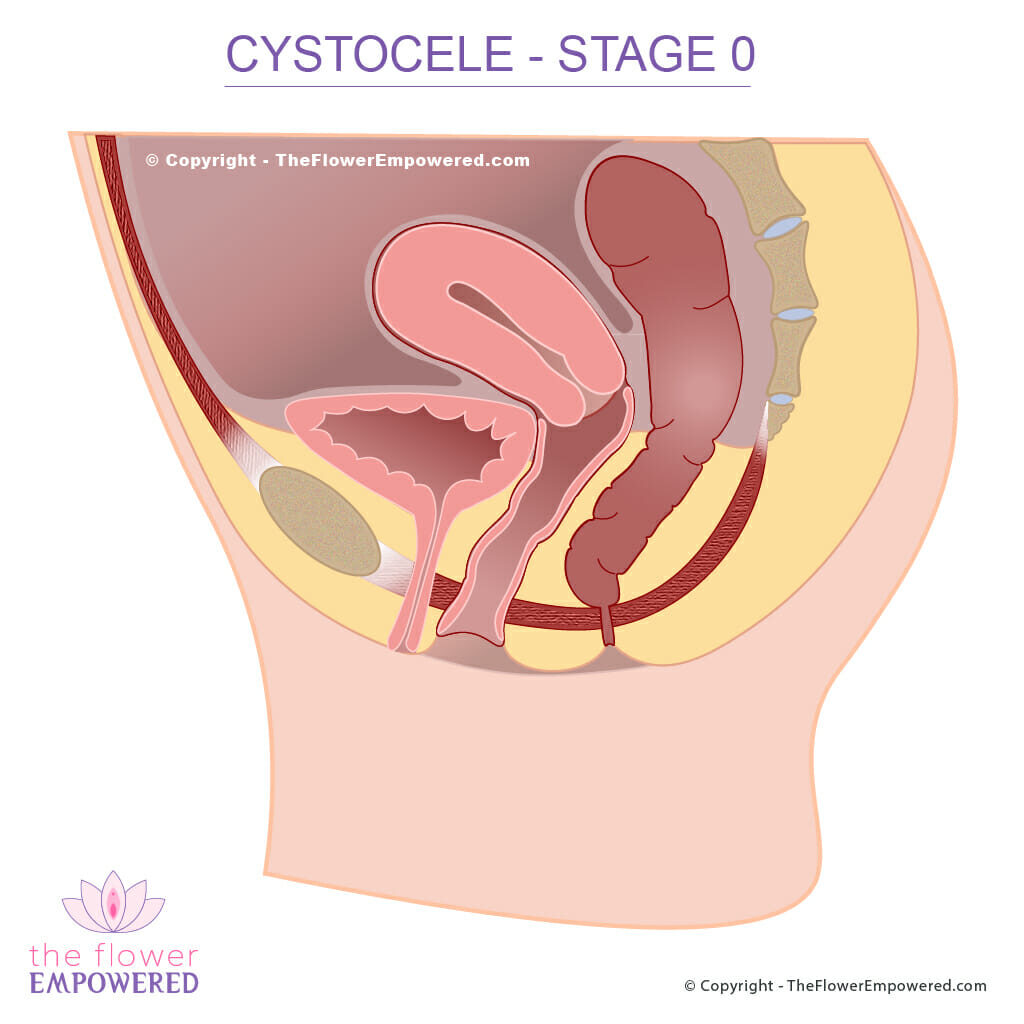
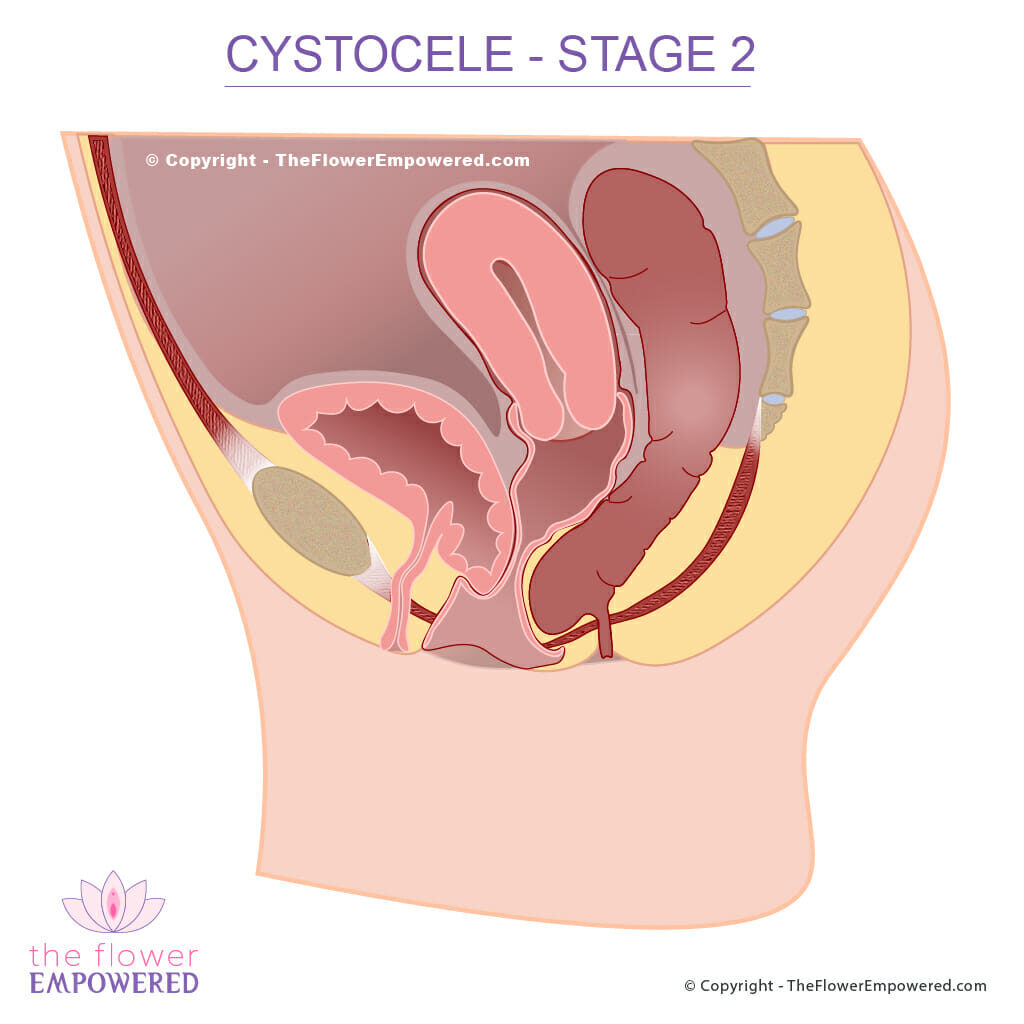
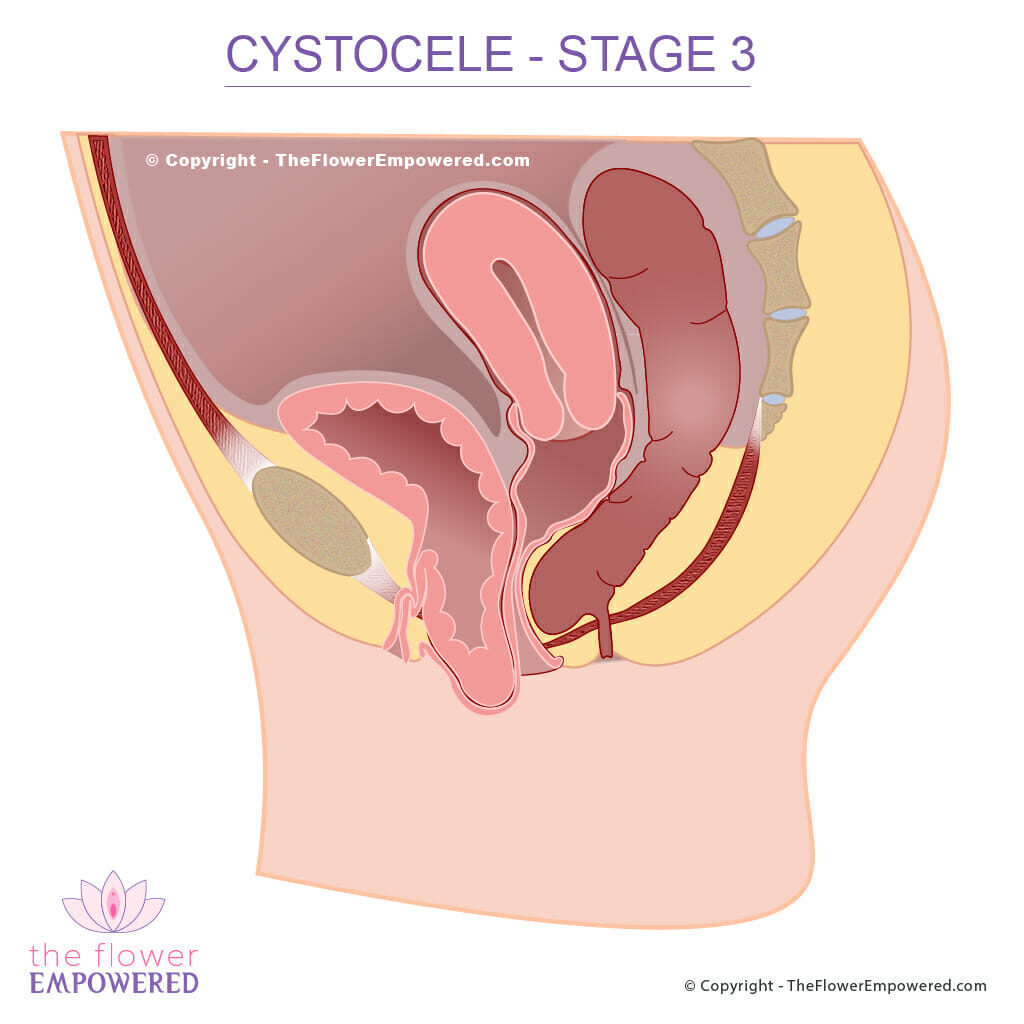
Bear in mind when looking at these images that they show the prolapse when under increased intraabdominal pressure. Without an increase in intraabdominal pressure, the organs and tissues do not generally bulge in the same way. In the case of severe prolapse, the bulge may be present at all times.
Stage 0 (No Prolapse)

Stage 1 (Mild Prolapse)

Stage 2 (Moderate Prolapse)
Stage 3 (Severe Prolapse)
Considerations When You Have Cystocele
If you are suffering from a prolapse, it is important to keep your stool soft and to prevent straining. Pelvic organ prolapses are an indication that the pelvic floor is sitting lower than it should, and that the connective tissue structures within the pelvis have been stretched. By working on increasing the strength and tone of your pelvic floor muscles, combined with hypopressive style exercises that work to enhance the relationship between the diaphragm and pelvic floor, you can make a positive difference to the grade of you prolapse. Connective tissue takes longer to repair than muscle fibres, but they do respond given sufficient time.
Make sure to avoid constipation as the bearing down when constipated can stretch the tissues further causing a worsening of your prolapse. You can find many videos on our YouTube channel giving tips on preventing constipation and demonstrating pelvic floor exercises and hypopressive techniques that if practiced consistently over time, will help to lessen your symptoms and improve the grade of your pelvic organ prolapse1.
Treatment for Cystocele
Like most symptoms of pelvic floor dysfunction, the treatment for cystocele falls into one of two categories; conservative (non-surgical) and invasive (surgical). Surgical options are generally only advised for severe cystocele (grade 3 or 4). For more information on the various treatments offered in these two categories, click on the relevant button below. If you did not find what you were looking for, you can search this site using the search bar at the bottom of the page.
Explore the Other Types of Pelvic Organ Prolapse
Having reviewed the Cystocele, you may be interested in exploring the other types of prolapse. You can do that from here:
References
- Bernardes BT, Resende AP, Stüpp L, Oliveira E, Castro RA, Bella ZI, Girão MJ, Sartori MG. Efficacy of pelvic floor muscle training and hypopressive exercises for treating pelvic organ prolapse in women: randomized controlled trial. Sao Paulo Med J. 2012;130(1):5-9. doi: 10.1590/s1516-31802012000100002. PMID: 22344353.