
Pelvic Floor Muscle Training Is an Effective Treatment for UI in Women1
Conservative Treatments for Urinary Incontinence
When it comes to non-surgical treatments for urinary incontinence, the options depend largely which type of incontinence is present. Generally, the primary treatment is pelvic floor muscle training (PFMT). However, if the symptom is stress incontinence, the focus is placed on strengthening the pelvic floor due to hypotonicity. In the case of overactive bladder, the focus is placed on pelvic floor relaxation combined with other treatments such as bladder retraining. On this page, we will review all of the treatments offered for the different types of urinary incontinence. You should always speak to your doctor or pelvic floor physical therapist if you have incontinence and they will guide you to the right treatments for you.
Regardless of whether your doctor suggests conservative treatments or more invasive surgical options, PFMT is always required. To have surgery without undertaking rehabilitation of your pelvic floor muscles is the equivalent to treating the symptom without addressing the root cause. Training your muscles will help to rebalance the pelvic floor to overcome hypertonicity or hypotonicity bringing the pelvic floor back to a normal resting state.
Pelvic Floor Muscle Training (PFMT)
The type of pelvic floor muscle training offered as the first line defense for urinary incontinence will be based on your incontinence symptoms. The symptoms depend on the type of pelvic floor dysfunction you have, which is explained on the pelvic floor dysfunction page.
Usually strengthening exercises (Kegels) are offered if you have hypotonicity (weakness). Alternatively, relaxation exercises (Reverse Kegels or “down-training”) are offered if you have hypertonicity (tightness).
Regardless of which type of pelvic floor training is offered, consistency is required. Strengthening a weak muscle or relaxing a hypertonic muscle will take time and repeated practice so make sure you put in the effort if you would like to see results.
Bladder Retraining
Bladder training is where you “positively program” your bladder taking advantage of your ability to control your sympathetic responses. Just like potty-training, this positive programming helps to return normal bladder function. An important part of bladder training is taking a baseline to establish where you are right now, and then tracking your progress over time. This is done using a bladder diary where you track your fluid intake and measure the volume of urine voided.
Each time you drink something, you need to measure the how much liquid you drink. When you urinate, you need to measure how much urine you void. You will need to have a measuring cup in the bathroom or a urine measuring pan (see the products section below) to collect and measure the volume of urine. If you are on the go, a Collapsible Measuring Cup will allow you to keep track of your urine when out and about. You can keep it in a sealable plastic bag and rinse it out after each use.
What Is a Bladder Diary?
Your bladder diary is a record of the volume of liquid that you drink and pee each day. You can record this information with pen and paper or alternatively, you can download an app. If you would like to use the paper method or are uncomfortable with logging your information in an app, we have created a printable pdf file which you can use
We have also created an editable version so you can still track digitally but your information is not stored anywhere but on your computer. The digital version will total your daily drink and urine volumes automatically. If you opt to use this digital version, save it to your computer and rename it each day with the date in the name so you have a daily copy.
Is PFMT Needed if I’m doing Bladder Retraining?
Pelvic floor muscle training plays an important role in bladder retraining which is a pivotal treatment for overactive bladder, even when you do not experience leakage. Contractions of the external urethral sphincter are an automatic response to the guarding reflex. If your bladder is sending signals to say that it is full before time, you need to tap into the guarding reflex. You do this by deliberately contracting your external urethral sphincter, which is a core component of a Kegel, the most basic pelvic floor exercise.
Additional Conservative Treatments for Urinary Incontinence
1. Bladder Retraining
Your bladder function is impacted by many factors, including your activity level. Studies have shown that health is negatively effected by sedentary lifestyles. In one study, they concluded that physical activity is associated with a decreased risk of bladder cancer. Whether you are striving for optimal health or trying to treat stress incontinence, overactive bladder or mixed incontinence, moving more should be of benefit. If you have a sedentary lifestyle, increasing your level of activity can help to reduce your level of incontinence. A Norwegian study found that “women who participated in low intensity activities for one hour or more per week had less incontinence than those who did not”.
2. Weight Management
Did you know that for every additional unit increase in your BMI, your risk of developing incontinence increases by 1%? Obese people have double the risk of developing incontinence. It’s not just the risk of incontinence that increases with wight gain, the severity also increases. Obese people are three times more likely to suffer severe incontinence than normal weight people. Lowering weight typically also lowers the severity. If your BMI is over 25, lowering your weight will help to decrease your intra-abdominal pressure which will have a positive effect on your incontinence. Diet plays a big role in weight loss/gain. It can be helpful to work with a nutritionist to help bring your weight back into the healthy BMI range. Movement also helps with keeping weight in check. Go walking with a friend or join a fitness class to help keep things in balance. As well as having a positive effect on your pelvic health, this should also improve your overall health.
3. Improve Your Posture
Your posture and alignment can directly impact the stability of your pelvic floor and should be assessed as part of your rehabilitation. One study found that “women with incontinence had more difficulty controlling their postural balance than continent women while standing with a full bladder. Therefore, developing therapeutic management focused on strengthening the women’s core muscles and improving their postural balance seems advisable“2 so it is advisable to follow a program that helps to rebalance your posture. Your physiotherapist or a structural integrator can help you to assess your posture. Postural assessment and exercises are included in the book Empower Your Flower.
4. Quit Smoking
Did you know that smoking more than 20 cigarettes per day increases your risk of developing incontinence? The smokers cough is believed to be a contributing factor. A study into the functional anatomy of the female pelvic floor with stress incontinence found that the intra-abdominal pressure from a sudden hard cough results in pressure on the pelvic floor requiring it to stretch by 1cm. This may not sound like much, but try to lift your pelvic floor by 1cm – not so easy, right? Each cough is like a little punch. If you keep punching your pelvic floor, you will weaken it. Smoking also impacts your autonomic nervous system. A 2015 study found that overactive bladder was common among smokers and female smokers significantly complained of nocturnal enuresis (bed-wetting) and coital incontinence (peeing during sex). If you are suffering from OAB, reducing the amount you smoke or quitting completely could have a positive effect.
5. Food Choices
The food you eat and liquids you drink can have a big impact on your bladder function. Many foods and drinks act as bladder irritants, such as spicy foods, sweeteners, caffeine, carbonated drinks and alcohol. You should limit your intake of these foods while you are treating urinary incontinence, and consider maintaining low intake of these foods once your symptoms have subsided. You also need to consider the impact of constipation, which negatively impacts your pelvic floor muscle function. Try to keep bowel movements between 3 or 4 on the Bristol stool scale. A diet high in fibre can help with this. You can work with a nutritionist to create a diet that works for you.
6. Reduce Stress
If you are under stress, it is likely that your parasympathetic nervous system is dominant, meaning your system is running in “fight or flight” mode. You may recall that your parasympathetic nervous system is responsible for contracting your bladder, while your sympathetic nervous system keeps it relaxed. A 2015 study concluded that patients with OAB reported psychological stress levels that were significantly higher than healthy participants. If you are consistently under stress, you should take active steps to reduce your stress levels. Try to spend time with people who make you feel positive and happy. Try to avoid stressful situations and add a daily meditation practice. You can use apps such as Calm for meditation. Gentle yoga is also good for reducing stress levels so maybe sign up to a local class or visit the relaxation playlist on our YouTube channel.
Medication for Incontience
Medication is sometimes offered to treat overactive bladder if conservative treatments are not producing the desired results. Medications to treat OAB have been used for decades but come with multiple side-effects including dry eyes and mouth. These symptoms can make you very thirsty, causing you to increase your intake of water. Drinking more than the recommended intake of fluid for one day (2.7 litres of 11.5 cups for females) can have a negative impact on the symptoms of OAB. Constipation is another common side effect, which can negatively impact the health of your pelvic floor. Additionally, Urinary retention/overflow incontinence can occur when taking these medcations
In some cases, Drugs for Overactive bladder are known as antimuscanarinic drugs. They work by inhibiting the neurotransmitters of PNS thus allowing your bladder to remain relaxed. The following drugs may be offered as treatment:
- Tolterodine
- Oxybutynin
- Trospium
- Solifenacin
- Darifenacin
- Miraberon
- Festorodine
Your urologist should prescribe the drug he/she believes will work best for you.
Neuromuscular Electrical Stimulation (NMES)
Another treatment option if you have urinary incontinence is Neuromuscular Electrical Stimulation (NMES). NMES, also referred to as ESTIM (Electrical Stimulation) uses an electric current to trigger muscle contractions. This type of treatment can be used for both stress incontinence and overactive bladder. However, the method of application is different for these types of incontinence. These treatments can generally be performed at home but should only be used under the guidance of your physical therapist (physiotherapist). Always follow the manufacturers instructions if you use one of these devices at home.
NMES for Stress Incontinence
With stress incontinence, NMES treatment is can be performed using an intravaginal probe, external skin electrodes, shorts with built in skin electrodes or by sitting on a specialized chair that produces a current through your clothing. The stimulation from NMES creates muscular contractions, but these contractions do not feel the same as those felt when contracting voluntarily. NMES generally recruits all muscle fibers with the stimulated contraction and for this reason, it is a favored treatment if the woman is unable to generate a strong contraction or cannot achieve any voluntary contraction. Studies into this treatment have shown varying levels of success, but it should be noted that NMES hadevices not been shown to be superior to PFMT, and if you are undertaking NMES, you will also need to do PFMT.
NMES Device With Vaginal Probe


NMES for Overactive Bladder
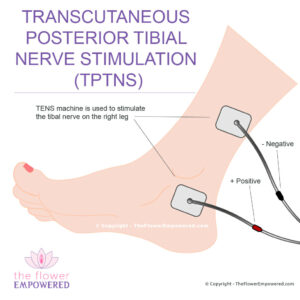
Transcutaneous Posterior Tibial Nerve Stimulation (TPTNS) is stimulation of the tibial nerve with skin surface electrodes. The treatment is preformed by placing two skin electrodes above and below the ankle where the tibial nerve is located. Treatment is typically for 20 minutes at a time and the duration between treatments varies from 3 days to one week. It is not yet understood how this treatment actually works, but there have been multiple small studies in the past decade that suggest that TPTNS is effective in the management of severe OAB. More larger-scale studies are needed. The stimulation device for TPTNS is the same as the device used for NMES, however, the settings used for this type of stimulation will be different.
Posterior Tibial Nerve Stimulation (TPTNS)
Invasive Treatments for Urinary Incontinence
Having reviewed the non-surgical treatments for urinary incontinence on this page, you may be interested in exploring the invasive options which include some minimally invasive options and some surgeries. Surgical options are generally only advised for once conservative options have been tried unsuccessfully for an extended period. For more information on the various treatments offered in these two categories, click on the relevant button below. If you did not find what you were looking for, you can search this site using the search bar at the bottom of the page.
Explore the Different Types of Urinary Incontinence
You can explore the different types of urinary incontinence from here.
References
- Radzimińska A, Strączyńska A, Weber-Rajek M, Styczyńska H, Strojek K, Piekorz Z. The impact of pelvic floor muscle training on the quality of life of women with urinary incontinence: a systematic literature review. Clin Interv Aging. 2018 May 17;13:957-965. doi: 10.2147/CIA.S160057. PMID: 29844662; PMCID: PMC5962309.
- Chmielewska D, Stania M, Słomka K, Błaszczak E, Taradaj J, Dolibog P, Juras G. Static postural stability in women with stress urinary incontinence: Effects of vision and bladder filling. Neurourol Urodyn. 2017 Nov;36(8):2019-2027. doi: 10.1002/nau.23222. Epub 2017 Feb 10. PMID: 28185317.