
Female sexual dysfunction affects 41% of reproductive-age women worldwide1
What Is Sexual Dysfunction?
Sexual Dysfunction is a recurring and persistent condition that impacts your ability to have a satisfying sex life. Female sexual dysfunction falls into four main categories: Anorgasmia, which is the inability to have an orgasm. Hypoactive Sexual Desire Disorder (HSDD), which is a loss of desire or low libido. Sexual Arousal disorder, which is an ability to become sexually aroused, and Dysparenia, which is pain during or following sex.
Sexual dysfunction negatively impacts quality of life. One US study found that sexual health was a highly important aspect when measuring quality of life, even for those who had poor health. If you are suffering from Pelvic Floor Dysfunction (PFD), the likelihood that you are experiencing sexual dysfunction is extremely high. A 2018 study found that sexual dysfunction was more prevalent among women with PFD2.
On this page, we will firstly explore normal sexual function including the role of the pelvic floor in orgasm. Secondly, we will review the causes of sexual dysfunction and we will discuss the specific sexual dysfunctions that are impacted by pelvic floor dysfunction, namely: dyspareunia and vaginismus.
Understanding Sexual Function
Normal sexual function generally follows a pattern beginning with desire, followed by arousal, leading to stimulation which builds up to orgasmic climax. Desire typically comes first, but not always. Maybe you can remember a time when you weren’t in the mood, but your partner did or said things to increased your desire creating arousal. Maybe your partner used stimulation to create arousal causing your desire to increase. Regardless of the route taken, if desire, arousal and stimulation are all present, you should be on the path toward an orgasm.
As the proceedings get underway, there are changes throughout the body. Heart rate and blood pressure increase. Pupils in the eyes dilate. Breasts swell up with the nipples becoming more sensitive and erect. The cheeks might flush. The blood supply to the vagina and cervix increases and the uterus can shift position, tipping downwards ready to welcome an inflow of sperm.
Is Penetration Needed for Orgasm?
Penetration isn’t required to achieve orgasm, in fact, orgasm can be achieved through clitoral stimulation alone. A 2018 US study into women’s experiences with genital touching, sexual pleasure and orgasm found that 36.6% of women reported clitoral stimulation was necessary for orgasm during intercourse. A further 36% reported having better orgasms if the clitoris was stimulated during intercourse.
The mechanism for touch, including location, pressure, pattern and rhythm is quite diverse between women. Understanding what works for you is pivotal to successful orgasm. A 2016 study found that for women, “partnered sex of good quality seems to promote cardiovascular health, specifically reducing the risks of hypertension“. Isn’t that a great reason to find a nurturing relationship where you are sexually satisfied?!
What Is an Orgasm?
An orgasm is the wonderful peak of a sexual encounter where your pelvic floor rhythmically contracts producing intense feelings centered in the pelvic region but often radiating throughout the body. Although your pelvic floor muscle contractions play a major role in orgasm, there is so much more at play than just the contraction of these muscles.


How Is Sexual Satisfaction Measured?
The quality of your sexual experience is very subjective. If you consistently fail to achieve orgasm during your encounters, you may report feeling unsatisfied. On the other hand, you may have really enjoyed the experience and feel no dissatisfaction on having failed to “cross the line”.
Your thoughts are influenced by the hormones that radiate through your body. Hormones play a major role in the sexual response cycle, where you go through phases of arousal, plateau of excitement, orgasm and resolution (the return of everything to normal following climax), and thus, hormones can impact orgasm.
The relationship with your partner (or yourself if you are masturbating) also has an impact on your sexual satisfaction. Your thoughts in their subjectivity have the ability to make your experience feel positive or negative. This is something we explore at length in the book.
What Is Happening Physically During Sex and Orgasm?
Aside from the obvious; stimulation, external, internal or both, and the reactions described above (dilated pupils, more blood to genitals etc), there are some other physical and chemical changes that are good to understand.
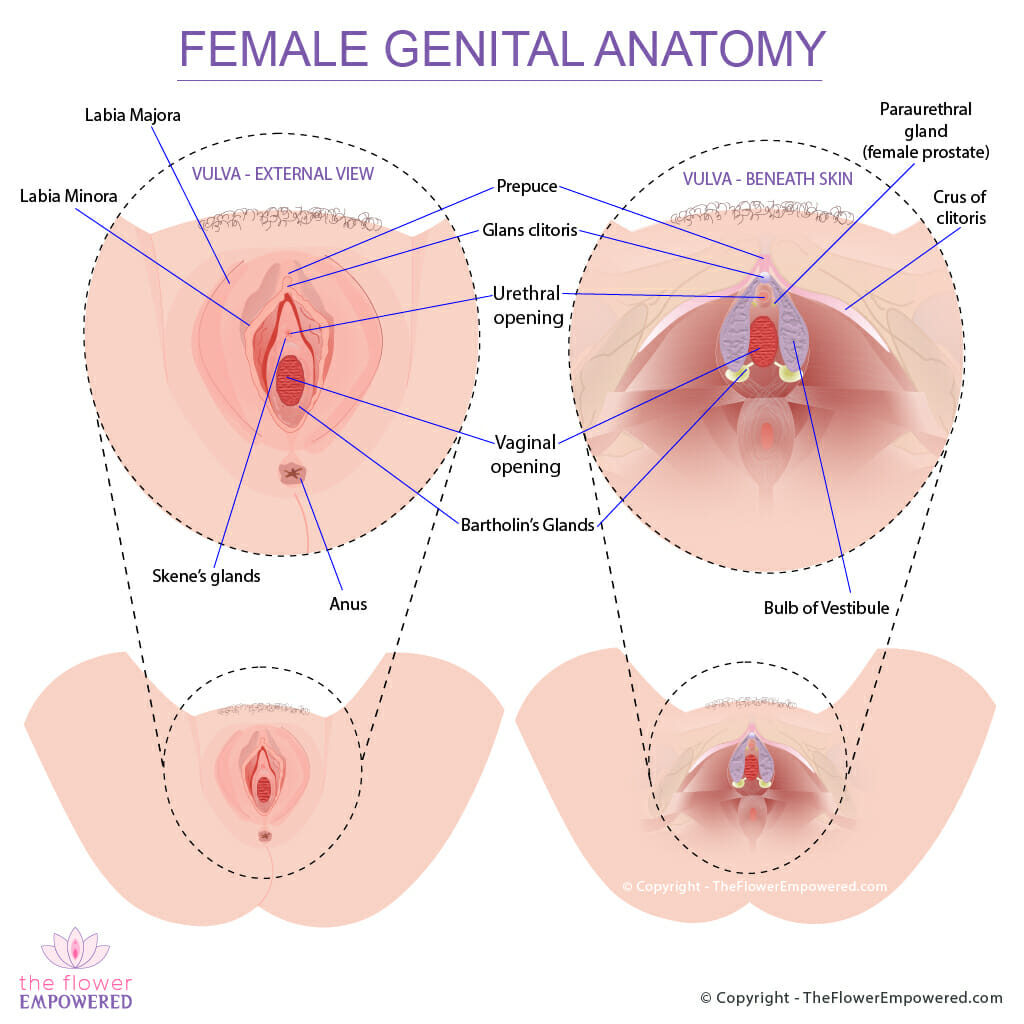
The diagram of female genital anatomy shows the external genitals (vulva) as well as the glands and muscles beneath the skin. When you experience arousal, the glands surrounding your vulva swell and create lubrication. Your Bartolin’s glands at the bottom of each bulb of vestibule secrete lubrication into the vagina making it wet to aide penetration.
The clitoris is not just the small bean shaped organ that you feel beneath your fingers, but is a much larger wishbone-shaped structure that measures about 9cm in length by 6 cm in width. The vestibules are composed of erectile tissue that surround the walls of the vagina.
The G-spot was objectively identified anatomically in a 2014 study. The 2014 study stated that it is an area “intimately fused with vessels, creating a complex” and concluded that the “G-spot presents as neurovascular tissues“. This was just one small study. Many other studies have failed to find the infamous g-spot.
Regardless of its definitive anatomical identification, women consistently confirm the existence of an area of heightened sensitivity a few centimetres in on the front vaginal wall.

When climax is achieved, there is rhythmic contraction of the pelvic floor muscles whilst the brain releases a cocktail of dopamine and oxytocin.
A portion of the front of the brain, that is responsible for self-evaluation, reasoning and control, is inactive during orgasm. This might explain in some way the release or “let-go” that is felt during climax.
What Is Squirting?
At the top of each bulb of vestibule, you have two small glands known as Skene’s glands which are the equivalent of the female prostate (paraurethral glands). The opening for these glands are very close to the urethral opening. These glands secrete liquid during sex and in some women, these glands can release fluid through female ejaculation. Female ejaculation happens in 10 to 54% of the female population. With female ejaculation, a few millimetres of thick milky fluid is expelled by the Skenes glands during orgasm. This is not the same as squirting.
Squirting is another phenomenon that is often combined with female ejaculation. In both cases, the secretions are from the Skene’s glands, however, in the case of squirting, the expulsion of tenths of millimetres of liquid comes from within the urethral opening. However, the liquid is not urine. It is defined as “a larger amount of diluted and changed urine”. Squirting is normally achieved by stimulating the g-spot (that infamous spot on the inside front wall of your vagina).
What Causes Sexual Dysfunction?
Sexual Dysfunction can be caused by pelvic floor dysfunction. If your pelvic floor muscles are either hypertonic (tight) or hypotonic (weak) when at rest, their ability to contract will be impacted which can result in weak or absent orgasms. Hypertonic (tight) muscles can also cause dyspareunia (pain during or after sex) or vaginismus (an inability to penetrate the vagina).
Of course, female sexual dysfunction is a complex condition and pelvic floor dysfunction is not the only. Many additional factors such as hormones, congenital issues, allergies, skin sensitivity, medications and psychological issues can impact female sexual function.
Another cause is pelvic surgery, which can damage muscles and nerves resulting in loss of sensation and/or pain. In cases where synthetic mesh or other materials are implanted into the vaginal area, there is an increased risk of developing sexual dysfunction. Particularly with synthetic mesh which has the potential to erode through the vaginal wall causing pain and in some cases, causing injury to the male penis.
Of the mesh implantation surgeries, mid-urethral strings pose the greatest risks to sexual function due to the placement in close proximity to the dorsal nerve of the clitoris while also being close to the crus of the clitoris. A 2015 study into the clitoris and its role in female sexual function highlighted the dangers stating that “The presence of a foreign body, such as with synthetic midurethral slings, can result in tissue reaction that may impact the nerovasculature of the vaginal wall and clitoris”. This is an important consideration if you are planning to have surgery with synthetic mesh.
Those who have sexual dysfunction linked to pelvic floor dysfunction will often suffer pain during sex. The diagnosis from pain during sex is typically one of four conditions – Vaginismus, Dyspareunia, Vulvodynia or Vestibulodynia.
With Vulvodynia and Vestibulodynia, the conditions relate to pain in the Vulva or Vestibule (odynia means pain). Although Vulvodynia and Vestibulodynia can be caused by PFD, the are more commonly caused by hormone imbalances, congenital issues, medication, or other medical conditions. If you have been diagnosed with Vulvodynia or Vestibulodynia, you can find out more by visiting the vulvar pain society website.
Sexual Dysfunction Conditions and Treatments
There are 2 main types of sexual dysfunction that are commonly caused by pelvic floor dysfunction: Dyspareunia and Vaginismus. You can read more about these conditions and their treatments by clicking on the buttons below. If you don’t find what you are looking for, just use the search bar at the bottom of the page to search this site.
Treatment Options for Sexual Dysfunction
Like most symptoms of pelvic floor dysfunction, the treatment for sexual dysfunction falls into one of two categories; conservative (non-surgical) and invasive (surgical). Surgical options are generally only advised for once conservative options have been tried unsuccessfully for an extended period. For more information on the various treatments offered in these two categories, click on the relevant button below. If you did not find what you were looking for, you can search this site using the search bar at the bottom of the page.
References
- McCool-Myers, M., Theurich, M., Zuelke, A. et al. Predictors of female sexual dysfunction: a systematic review and qualitative analysis through gender inequality paradigms. BMC Women’s Health 18, 108 (2018). https://doi.org/10.1186/s12905-018-0602-4.
- Dheresa M, Worku A, Oljira L, Mengistie B, Assefa N, Berhane Y. Pelvic floor disorders associated with higher-level sexual dysfunction in the Kersa district, Ethiopia. Turk J Obstet Gynecol. 2018 Dec;15(4):210-216. doi: 10.4274/tjod.86658. Epub 2019 Jan 9. PMID: 30693135; PMCID: PMC6334248.