



Estimated reading time: 22 minutes
Pelvic mesh removal surgery is considered to be major surgery carrying with it many risks. As a member of the global mesh community, I hear from women every day who have undergone pelvic mesh implantation only to suffer serious complications afterwards. The rate of complication following pelvic mesh implantation is 1 in every 10 women for both incontinence mesh and pelvic organ prolapse mesh. With such high rates of complication, it’s no surprise that many women are asking for pelvic mesh removal surgery. Unfortunately, these mesh devices were designed for permanent implantation making removal a real ordeal. In this article we will explore the complications caused by pelvic mesh and discuss why doctors are afraid to perform pelvic mesh removal surgery. We have compiled a list of 18 considerations for those who are planning to have pelvic mesh removal surgery.
My surgeon had explained that there were no risks with the device and that surgery was very commonly performed giving almost 100% success rates. If you visit a surgeon today, you will most likely hear that same story – mid-urethral sling is the “gold standard” with almost 100% success rates – is that a lie? Not exactly. This quote, based on biased trials, focuses on the “objective” cure rate. I was deemed to be “objectively cured” following my surgery. Whereas I didn’t experience a single episode of stress incontinence during the one and a half years I had TVT mesh in my body, I instead suffered a range of debilitating symptoms that made every day a living hell. Was I objectively cured? Yes, however, subjectively, my life was ruined. You can read more on objective and subjective cure rates on the Pelvic organ prolapse and stress incontinence pages.
The Journey That Started With the “Gold-Standard”
Just over three years ago, I had pelvic mesh removal surgery to remove a TVT mesh sling that had been implanted to support my urethra to treat mild stress incontinence. My incontinence was very occasional (typically when sprinting to the finish line during a half marathon distance race) but my surgeon felt it would be a good idea to implant the “gold standard” TVT sling while I was having an operation to repair my perineum and a stage 1 rectocele (a type of pelvic organ prolapse). The TVT mesh, a type of mid-urethral sling, was going to ensure I would never have a leak again – perfect!!
My surgeon had explained that there were no risks with the device and that surgery was very commonly performed giving almost 100% success rates. If you visit a surgeon today, you will most likely hear that same story – mid-urethral sling is the “gold standard” with almost 100% success rates – is that a lie? Not exactly. This quote, based on biased trials, focuses on the “objective” cure rate. I was deemed to be “objectively cured” following my surgery. Whereas I didn’t experience a single episode of stress incontinence during the one and a half years I had TVT mesh in my body, I instead suffered a range of debilitating symptoms that made every day a living hell. Was I objectively cured? Yes, however, subjectively, my life was ruined. You can read more on objective and subjective cure rates on the Pelvic organ prolapse and stress incontinence pages.
Mesh Complications
For me, the complications included urinary tract infections, chronic cystitis symptoms (constant need to urinate, burning sensation when urinating, only peeing a few drops) as well as painful intercourse (dyspurenia). Sounds terrible, but believe it or not, I was one of the lucky ones. I could still walk and do yoga. I had to stop running after a few months as it really irritated my bladder (no more sprint finishes for me!!). You can see a list of mesh complications below:
- Urinary Tract Infection
- Mesh Erosion
- Pain (walking, sitting, resting)
- Dyspurenia (painful sex)
- Hispurenia (mesh hurting your partner during sex)
- Cystitis
- Voiding difficulty (can’t pee)
- Abscess or infection
- Autoimmune diseases
- Fibromyalgia
- Constipation
- Vaginal discharge
- Antibiotic resistance
- Nerve damage
- Organ perforation
- Low back pain (concern if sacrocolpopexy)
- De-novo incontinence (a new incontinence)
- Recurrent incontinence (return of old incontinence)
- Recurrent Pelvic Organ Prolapse (POP)
- Depression and Anxiety
My Mesh Removal
At first I didn’t think mesh was to blame for my issues, after-all – it was the “gold-standard”. In an attempt to relieve my symptoms, I changed what I drank, changed my diet, reduced my movement and planned my life around the nearest toilet – all to no avail. Eventually, when every other possible cause was eliminated, my surgeon agreed that the symptoms were due to the TVT mesh. He could just remove it right? Wrong!! Whereas he was trained to perform the 15 minute surgery to implant the device, he was not trained to remove it! Does this sound insane to you or is it just me?? Not only are surgeons not trained to perform pelvic mesh removal surgeries, until recently they had been given little to no advice on the management of adverse events and complications. This goes some way to explaining why surgeons seem so lost when you present with complications!


Treatment and Management of Mesh Complications
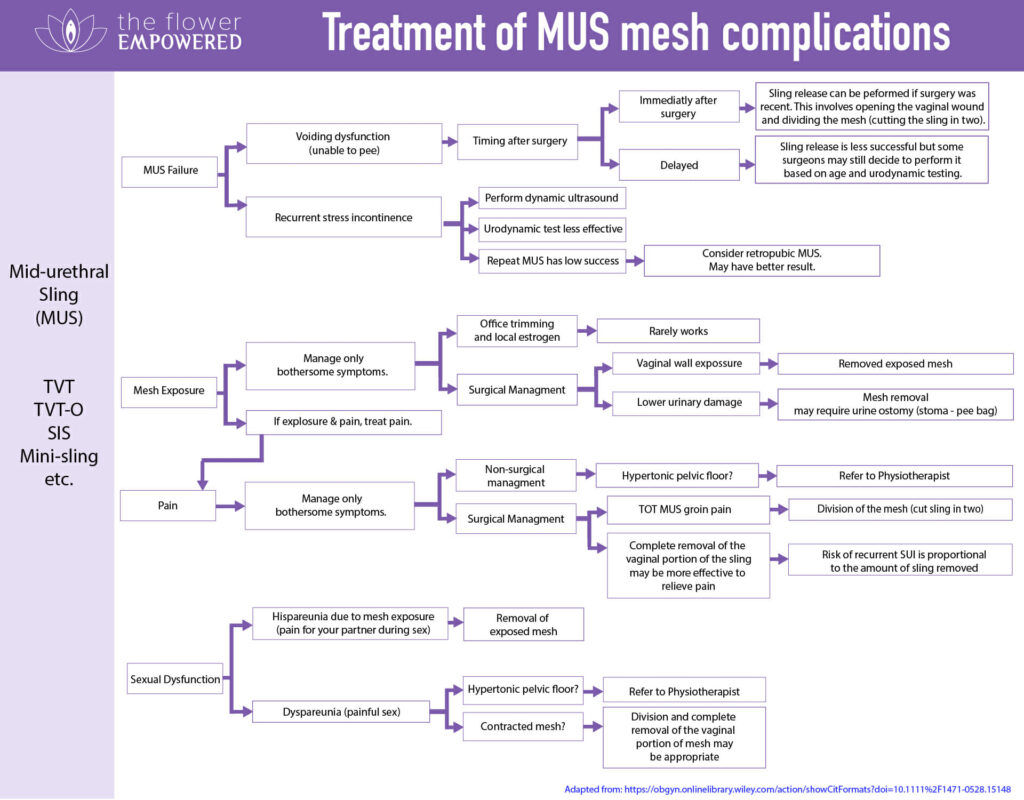
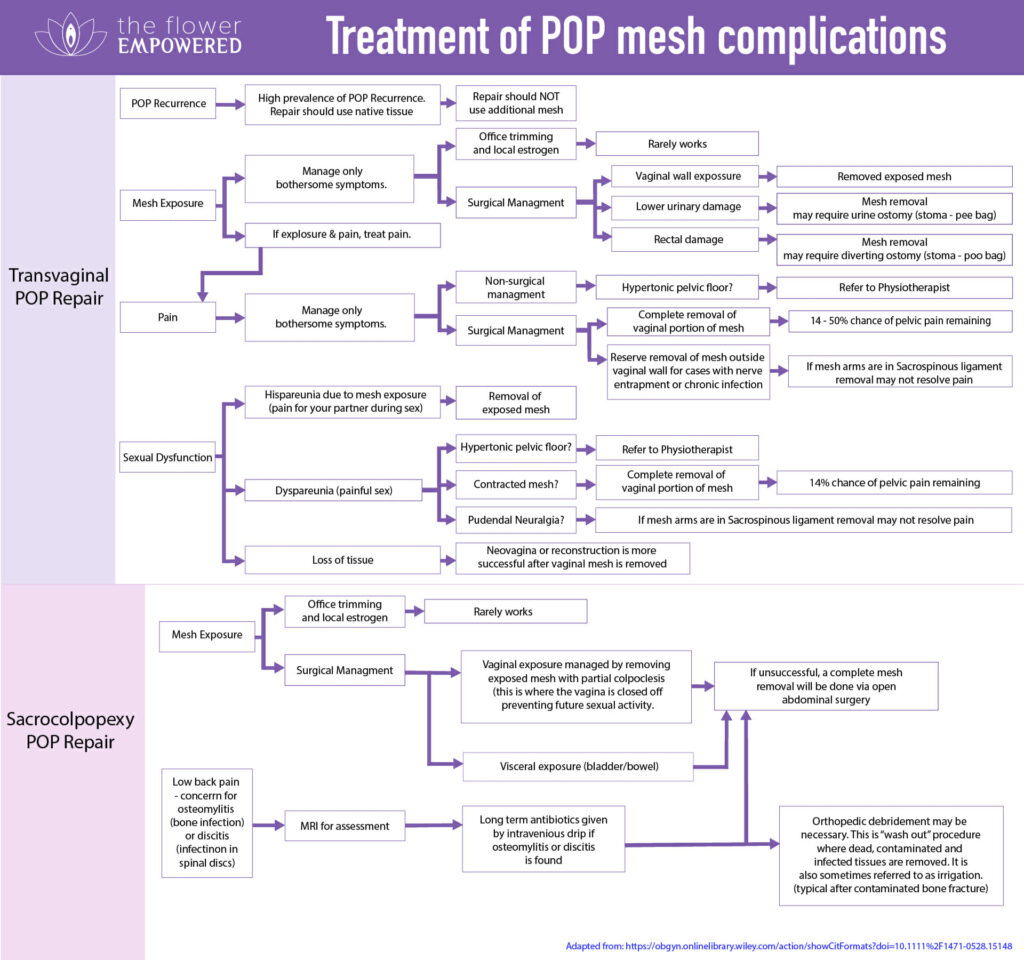
So what are the treatment options? In light of controversy surrounding these mesh devices (see 60 minutes documentary, Sky News in UK, W5 in Canada, ABC News in Australia and the Netflix documentary The Bleeding Edge) combined with the growing evidence of high rates of complications, research is starting to focus on mesh complications and what to do when things go wrong. A group of OBGYN researchers from Canada, South Africa and UK published a study in March of 2018 offering an evidence-based method for managing pelvic mesh complications. The objective of the study was to “develop a treatment algorithm for the management of mesh complications” while identifying the gaps in literature and training.
In the discussion, they highlighted that “products were marketed with inadequate safety studies because their regulatory approval was based on the FDA 510 mechanism, eliminating the requirement for safety and efficacy data for Class II devices with a prerequisite device”. Depressing reading if you are one of the many women suffering pelvic mesh complications. The output of this study was a treatment algorithm (in lay-man’s terms, this is a flow chart) to be used by medical professionals when dealing with mesh complications. I have created “lay-man’s” versions of these flow-charts so you can see what your surgeon is likely to go suggest as your treatment options.
You will notice that none of these flows lead to a “happy ending” and hardly any suggest full pelvic mesh removal. Pelvic mesh implants are designed for fast and permanent implantation. This allows more surgeries to be performed per surgeon per day making it very profitable for surgeon, hospital and mesh manufacturer. Implantation is often “blind” meaning the surgeon cannot see where the large implantation needles (trochars) are going. This blind invasive implantation through the heavily occupied space of the pelvis carries risks of injury during implantation (e.g. bladder or bowel perforation) as well as the risk of mesh-based complications following surgery. During the design of mesh devices, thought was given to fast implantation methods, however, no consideration was given to removal.
You will notice that none of these flows lead to a “happy ending” and hardly any suggest full pelvic mesh removal. Pelvic mesh implants are designed for fast and permanent implantation. This allows more surgeries to be performed per surgeon per day making it very profitable for surgeon, hospital and mesh manufacturer. Implantation is often “blind” meaning the surgeon cannot see where the large implantation needles (trochars) are going. This blind invasive implantation through the heavily occupied space of the pelvis carries risks of injury during implantation (e.g. bladder or bowel perforation) as well as the risk of mesh-based complications following surgery. During the design of mesh devices, thought was given to fast implantation methods, however, no consideration was given to removal.
If you follow the various flows in these charts, you will see many suggest division or partial removal. Many women who undergo division or partial removal of pelvic mesh will have repeat surgeries due to continuing issues. With so few studies exploring the outcomes of pelvic mesh removal, it’s hard to know what to expect.
In my case, I decided not to have a division or partial removal, even though I knew that full pelvic mesh removal would leave me completely incontinent. The decision to have mesh removed (like the decision to have it implanted) is not to be taken lightly. Having only one mesh made my decision easier. My pain stopped the very day the mesh was removed. Unfortunately this is not true for everyone. Let’s explore the 18 considerations that I believe are key if you are planning pelvic mesh removal.
18 Considerations When Planning Pelvic Mesh Removal Surgery
As well as planning the surgery, it is important to have a plan for your preparation and recovery. Traveling a long distance for surgery is far from ideal but it is often required. We cannot know what complications may arise during surgery, or in what shape we will be following surgery, so forward planning will ensure you are prepared for many of the possible eventualities.
1. Finding a Pelvic Mesh Removal Surgeon
Before you can plan a pelvic mesh removal surgery, you need to find a pelvic mesh removal surgeon! Finding a local surgeon experienced in pelvic mesh removal may be difficult. Many women are required to travel long distances to have surgery (from Europe to USA for example!). In my case, I traveled from Sweden to Oxford, UK where Dr. Natalia Price performed a complete laparoscopic removal of my TVT mesh. The most commonly mentioned pelvic mesh removal surgeons are Dr. Raz, Dr. Veronikis and Dr. Elneil, however, I cannot recommend which surgeon is the best choice for you. Do some research, speak to others in the mesh community and use the surgeon who you feel offers you the best chance of success.
- Dr. Raz, USA
- Dr. Veronikis, USA
- Dr. Elneil, UK
- Dr. Price, UK
- Dr. Smith, USA
- Dr. Lee, USA
- Dr. Walker, USA
- Dr. Patel, USA
- Dr. White, USA
- Dr. Zimmern, USA
- Dr. Orejuela, USA
- Dr. Siddiqui, USA
- Dr. Porter, USA
- Dr. Gupta, USA
- Dr. Margolis, USA
- Dr. Mc Crery, USA
- Dr. Francis, USA
- Dr. Klingele, USA
- Dr. Kohli, USA
- Dr. Butrick, USA
- Dr. Fenner, USA
- Dr. Vogt, USA
- Dr. Summitt, USA
- Dr. Ellington, USA
- Dr. Parnell, USA
- Dr. Speights, USA
- Dr. Diaz-Valentin, USA
If you are aware of any additional surgeons that you believe should be on this list, please get in touch!
2. Type of Pelvic Mesh Implant
Removal of the uterus, particularly when the cervix is also removed, impacts on the stability of the ligaments of the uterus. Hysterectomies have been practiced since 1813, and many techniques have been developed to re-stabilise these support structures following uterus removal. Hysterectomy is often performed for medical reasons, however, it has become routine practice to remove the uterus during uterine prolapse repairs, even though the risk of subsequent prolapse is high (between 10 – 40%).
POP is one of the the three most common reasons for performing a hysterectomy. The uterus itself is not typically the cause of prolapse, so removal without a good medical reason should be questioned. Some studies indicate that hysterectomy could accelerate menopause by compromising the flow of blood to the ovaries. Taking all of these things into consideration, the decision to remove the uterus without a valid medical reason should not be taken lightly. If you have a hysterectomy, there is a great support forum online called Hystersisters.
3. Type of Mesh Anchors
If the device has anchors or staples which embed in muscle or bone, these can also prove difficult to remove while increasing the risk of pain remaining post removal (up to 50%). An example of a Pelvic Organ Prolapse surgery which includes staples is the sacrocolpopexy. Sometimes, sacrocolpopexy mesh covers the entire vaginal wall and removal requires rebuilding the vagina. The sacrocolpopexy uses titanium stables which attach it to the sacrum bone at the base of the spine which can also be a site of infection resulting in serious complications.


4. Unexpected Mesh Erosion
A 2014 study into operative management of mesh complications (90 patients) found many cases of unexpected mesh erosion into a second area during the removal surgery (5% in the vagina, 1% in the bladder and 2% in the bowel.) The patient with the unexpected bladder erosion required a further surgery to repair the bladder. These types of complications can arise during surgery and there is a risk that you may require a stoma (pee bag or poop bag) if damage is extensive. There is also a risk that your surgeon could accidentally perforate an organ when trying to remove mesh. An unexpected issue like this can significantly impact your recovery.
5. Removal of Mesh Doesn’t Always Equal Removal of Pain
In that same 2014 study, pain symptoms remained in 49% of the women following pelvic mesh removal. It should be noted that 39 of the 90 women had undergone at least one prior mesh revision surgery and that post-surgery follow-up for most patients was less than 6 months. Each surgery brings with it new scar tissue and potential for further injury/pain. Recovery from your first mesh surgery could be significantly different from second and subsequent surgeries. Joining a mesh support group and talking with women who have been through the same procedure, maybe even with the same doctor, could help when making the decision to have a removal.
6. Your General Health
If you have other health conditions in addition to those caused by mesh, this can make pelvic mesh removal surgery more complicated (e.g. diabetes or obesity). It is best to address your general health before going for removal surgery. This can be one of the biggest challenges, but one that should give you the best chance of having a smooth recovery.
7. Book Assisted Travel
If you need to fly for your pelvic mesh removal surgery, I cannot emphasise enough the importance of booking assistance for your home-bound journey. Most airlines offer assistance free of charge. As part of this service, you will be collected from check-in and taken with your bags all the way to your car when you reach your destination airport. This is important as you will not be able to lift your bags or to walk far following surgery.
If you are traveling alone, make sure to arrange for your partner, family member or friend to meet you at your home airport. In some airports, you are required to wait until the flight is almost completely boarded before they collect you from the special assistance area. Other airports may collect you immediately when you check-in taking you directly to your gate. You can ask your airline how they deal with special assistance when you call to make the arrangements. Make sure to arrive with sufficient time for the airline to assist you from check-in to your gate.


8. Don’t Rush Home Too Soon
We all want to return to the comfort and safety of our own home as soon as possible following pelvic mesh removal surgery, however, you should give yourself at least a week before you travel back. Flying soon after surgery increases your risk of developing deep vein thrombosis (particularly if you are taking a long-haul flight). Sitting in the same position for a long time, particularly if you have stitches around your vagina or urethra, can increase your pain levels. Long haul flights can also cause constipation, so you should ensure you take a stool softener before and after flying and keep yourself hydrated during the flight. Stocking up on your pain meds before you travel is beneficial, although the hospital will most likely provide you with sufficient meds for the week or two following surgery.
9. Bring Someone With You
This is easy to say, but harder to do. Discharge from hospital following pelvic mesh removal surgery is generally a day or two after your surgery. This is a very short time and you will not be fit to carry bags or to walk far. Ideally, you will have a family member, your partner or a friend traveling with you. Of course, this greatly adds to the expense, particularly if you have traveled across the Atlantic. If you are unable to bring someone along and you don’t know anyone in the area, reach out to the mesh community, to see if someone lives close by and can help you in those first days. Otherwise, use services like Uber to take you from door to door. Use a hotel rather than an Airbnb so you can have your bags carried from the car to your room and call on room service to bring you food and other necessities.
10. Flying After Surgery
During most surgeries, you will be given surgical stockings to maintain blood circulation in your legs during surgery. Check with your surgeon before you travel to ensure you will receive these stockings and if not, buy a pair before you leave.
Make sure to wear your surgical stockings during your flight and get up for a short walk every hour during the flight. This should minimise your risk of developing DVT. You can also do some ankle exercises while seated. Many long-haul airlines show relevant exercises in the inflight magazine.

11. Flying With a Catheter or Stoma
If you still have a catheter in place when flying home, mention this to your airline before going to the airport. The airline can ensure that you are seated in an aisle seat close to toilets. If you are traveling through USA, you can print a TSA Notification card allowing you to discretely notify the TSA agent of your catheter or stoma bag. They may need to do a security screening including a pat-down with your bag on the outside.
You have the right to request a private screening showing your TSA notification card to explaining the reasoning. I suggest you print the TSA Notification card before you travel just in case it is needed. It is also important to check with your surgeon and catheter/stoma manufacturer to ensure that the bag is safe and durable for air travel. A ruptured bag due to cabin air pressure is something you shouldn’t have to deal with during your flight home.
12. Urination Following Surgery
It is impossible to know how urination will function following surgery. In the worst case, you may be fitted with a urine stoma – a permanent pee-bag that you will use to empty your bladder for the rest of your life. In most cases, your surgeon should an inclination if this may be required before you have your surgery, so make sure to discuss it. Waking up to find a stoma can be quite a shock if you have not already considered the possibility. You can read more on living with a urine stoma on the Urostomy association website.
In many cases, a catheter is left in place for a few days following surgery. A catheter is a bag with a small tube attached which is inserted into the urethra to empty the bladder. When the catheter is first removed, you will have a trial period without the catheter (TWOC) during which you will see if it is possible to urinate spontaneously. You can return home during this trial (or to your hotel room if you have traveled for surgery). You may need to self-catheterize if urination doesn’t happen during this trial period.
I didn’t need catheterisation following my surgery. Initially, I was able to pee “on demand” (which was very frequently). Peeing felt very different following surgery, almost as though the urine was falling out of my body with no pressure behind it. I initially believed that I was going to be continent, but as the swelling went down, I learned that not to be true. It took me 18 months to regain my continence. As well as using pelvic floor muscle training to rebuild my pelvic floor, I had to retrain my bladder to overcome the overactive bladder symptoms.
13. Diet and Nutrition (& Poop)
What you eat following pelvic mesh removal surgery impacts the consistency of your poop and can cause constipation. Believe me when I say, you do not want to be constipated following pelvic mesh removal surgery! If you do become constipated you will end up straining to poop, which can pop a stitch or cause a new prolapse to manifest. The two weeks following surgery are critical from a poop perspective. Relaxing your anal sphincter to allow the poop to leave your body is a real challenge, and one that you must master.
It is best to consume a diet that keeps your poop measuring type 3 or 4 on the Bristol stool scale. I got this wrong following my surgery by taking a strong stool softener to keep my poop soft. I ended up on the opposite end of the poo spectrum with diarrhoea which also causes an involuntary straining along with excessive pooping. To resolve this, I stopped taking the stool softener and opted instead to add ground flax seeds to some fruit and yogurt. This helped bring balance back to the consistency of my poo.
Everybody is different so investigate what diet produces the perfect poo for you before you have your surgery and run with that diet in the weeks following removal. In the longer term, you need to consider a diet that promotes muscle growth when combined with a program of pelvic floor rehabilitation.


14. Vitamins and Minerals
Have your bloods tested before surgery to check for vitamin and mineral deficiencies. Supplementing for deficiencies can help optimize your chance of successful recovery. Make sure to check with your doctor before taking supplements as some may interfere with other medications used in surgery. I found that I was low in Vitamin D, B12 and zinc and Iron so I supplemented these along with Vitamin C (for iron absorption), magnesium ( for bowel function) and iodine (to kill fungus and bacteria). Taking probiotics is also advisable as you will be infused with high dose antibiotics during surgery which can kill a lot of your healthy bacteria. A probiotic can help to re-populate your microbiome with healthy bacteria thus boosting your immunity.
15. Sleep
It is believed that the body repairs during sleep so it is important to get good sleep following pelvic mesh removal surgery. In the first days and weeks, listen to your body. It will tell you when it is time to sleep. You will most likely sleep more than normal in the first days with sleep starting to normalize again after two or three weeks. If you can take these weeks off work, that will allow you to sleep without an alarm. If you have small kids, have your partner, family member or friend stay to care for the kids while you get your much needed rest.
16. Lower Your Expectations
This sounds negative, but it will positively impact your recovery! If you have high expectations of returning to work soon after surgery and bouncing around the house doing your normal activities, you are more likely to push beyond your capabilities causing injury. My yoga practice helped immensely in the days following my surgery. By this, I do not mean that I practiced yoga postures, that’s not it at all! In yoga, we practice acceptance and non-violence (ahimsa) which is something we also need to practice following pelvic mesh removal surgery. You will meet a different version of your body after surgery.
Listening to this new version of your body each day and accepting what you meet will help to get you through those first tough days and weeks. When you can accept what you meet, you can gently explore what is showing up in your body. If you push yourself to go back to work, to lift your kids, to hoover the house or to carry the shopping before your body tells you that it is ready, this is the equivalent to being violent towards yourself. Before surgery, tell your partner, family and friends that you will need help and be prepared to keep asking for help in the days and weeks and months following surgery.
17. Keep Calm and Breathe
In my opinion, this is one of the most important considerations, both before and after pelvic mesh removal surgery. You may be worried and apprehensive before your surgery. A calm steady state keeps your sympathetic nervous system active – that’s the rest and digest system which helps with recovery.
If you are anxious and panicky, your parasympathetic nervous system will dominate – that’s your fight or flight system. Try to keep stress levels to a minimum and find your happy place within. Flying after surgery can generate worry – I know this as I had to take a 9 hour flight 9 days after surgery. I meditated during my flight and worked to keep my thoughts on the positive side of the thought spectrum rather than jumping to fear with every little pain and twinge.
You can use an app such as Calm to help you relax. The app offers many different meditations. Breathing can also help to calm your nervous system. Taking long inhales with extended slow exhales taps into your sympathetic nervous system tricking your body into calming down when you start to feel panicked.


18. Slow and Steady Wins the Race
Following any pelvic mesh removal surgery, you will need to undertake a program of rehabilitation that recreates the connection between your brain and your pelvic floor. Your nerves may have been damaged by the mesh and subsequent removal surgeries. Your muscles are most likely in a combination of hypertonicity (overly tense) and hypotonicity (lax and weak). Identifying the state of your pelvic floor and performing a baseline assessment is one of the first steps detailed in the book which covers recovery from the absolute beginning – where you may have little to no sensation or strength, to a place of great strength builds where you can ride horses, go running and skipping and do star-jumps! It is important to give yourself time. Rome was not built in a day. A strong foundation will not be created overnight. Consistency will be key to your success in the journey to empower your flower.
If you want to know the impact of mesh, ask the patients! That is exactly what we plan to do. If you have a mesh device implanted to treat incontinence or pelvic organ prolapse, we need your feedback. If you have already had a mesh removal, your feedback is also valuable.
My doctor told me I could go back to work 5 days after my mesh removal. Does this seem right? I’m 2 days post op and definitely not thinking I should go back to work Monday. I can’t find any info on returning to work after mesh removal surgery. Thoughts?
hi i am looking for advice on a surgeon in the US that maybe one of you have used for mesh removal i am in my early 30s and nervous about mesh removal.
Thank you for all this information
I had a TVT sling put in on 7/14/21, surgery to recover vaginal erosion 10/22/22 and removed the whole sling due to exposure 2/11/22. I was also told this was the ‘gold standard’. It’s near to ruined my life the last 9 months. If only I’d just had the prolapse surgery and no midurethral mesh inserted. At least my same surgeon could take it out. Since then the vaginal scar tissue and nerve damage has become an issue and a partial prolapse has returned which pushes the scar tissue near to outside my vaginal opening. I’m so tired of surgeries, but I think I need vaginal reconstruction now to regain sexual function and not have discomfort from scar tissue so close to outside my body and where I sit. I’m scared to get another surgery though. I also need to wait for awhile after having 3 surgeries in a year.
I just had mesh removal 3/24/22 and am unable to walk correctly. Pain in leg leg along with weakness. Is this normal?
It can be. Very much depends on the type of mesh. If it was TVT-O, it would have been passed through some of the muscles in your legs so you might have some pain and weakness in the legs initially. Has it rectified itself already?
Hi, I hace a mesh complication the mesh exposure, please what doctor Is the best un usa near me Florida, please sent a email seria.ponce@gmail.com my problem have 7 month
Unfortunately I can’t recommend specific doctors. You may be able to get recommendations from someone in your local area if you join a local mesh support groups. You can find groups here: http://theflowerempowered.com/pelvic-mesh-support/
I had the TVTO procedure in 2004 and now I have a non healing vulvar wound from abscess and possible osteomyelitis from mesh erosion and another abscess. I need mesh removal and any suggestions for Physicians would be appreciated. (Someone who does them frequently). Dr Miklos , Ga. was suggested. I live near Fort Myers, Florida Thank you
I live in Pennsylvania do you have any good surgeon to remove bladder slings. Near me
Hi Kathleen, I can’t recommend any specific mesh removal surgeons in US as I have only personally had experience with one and she is based in UK. Sorry!
I received another tip – book a business class ticket on your home-bound journey if you are traveling long haul.
This way you can lie down during the flight. I also forgot to mention some key things to watch out for in those days following surgery: Fever, chills, vomiting, an increase in the level of abdominal or pelvic pain, redness or swelling around incisions. Puss or bleeding from incisions. Swelling and pian in one leg. Stinging and pain during urination. If you have any of these issues you should contact your surgeon promptly.
I’ve received a few questions on when to return to exercise and when to have sex. Your surgeon will advise you on these matters. I started gentle yoga after two weeks and slowly increased my movement as my body allowed. Points 16, 17 and 18 above should be kept at the front of your mind when resuming activities. Take it slowly, listen to your body and don’t expect too much too soon (this goes for exercise and having sex!!). Hope this helps 🙂 <3