



Estimated reading time: 5 minutes
In the first of our Let’s Talk About series on YouTube, we explore vaginismus. Vaginismus is a form of pelvic floor dysfunction that causes the pelvic floor to involuntarily contract when vaginal penetration is attempted. It can feel as though there is a wall blocking the entrance, which can strike fear into your heart as this is completely outside of your control. With between 5 and 17%1 of women being impacted by the condition, it is critical that we talk about it.
In its primary form, vaginismus can prevent penetration when first using tampons or trying to insert a menstrual cup. It can also prevent penetrative sex. For this reason, primary vaginismus is generally discovered during puberty or in early adulthood. The secondary form of vaginismus can occur following childbirth, during menopause or following pelvic surgery or trauma. That trauma can be physical or chemical in nature (such as a bad fall, radiotherapy for cancer treatment or an infection).
Lastly, there is a spontaneous form of the condition which can happen at any point in life. This spontaneous is the body’s natural defence mechanism if penetration is forced, but it can also occur when a tampon or vaginal weight is being used. In that instance, the pelvic floor involuntarily contracts preventing removal of the weight or tampon. This is not considered true vaginismus as it’s not a chronic condition and can generally be resolved without extended treatment.
How Can You Tell if You Have Vaginismus?
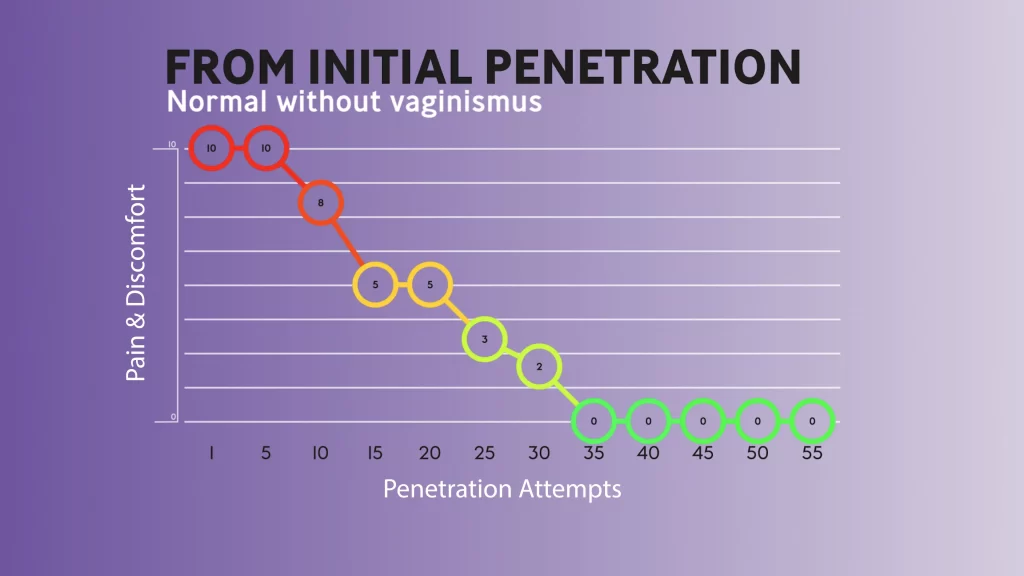
Many women mistakenly believe that the initial difficulties, discomfort and pain when first using tampons or trying penetrate sex is vaginismus. It is normal to have some discomfort and pain when you first attempt penetration but it typically resolves over time with practice. In the case of vaginismus, there is no progress even with repeated practice. This is highlighted in the following two graphs. The first shows how discomfort and pain are reduced under normal circumstances as penetration is practiced.
Normal Response to Penetration
The first shows how discomfort and pain are reduced under normal circumstances as penetration is practiced.

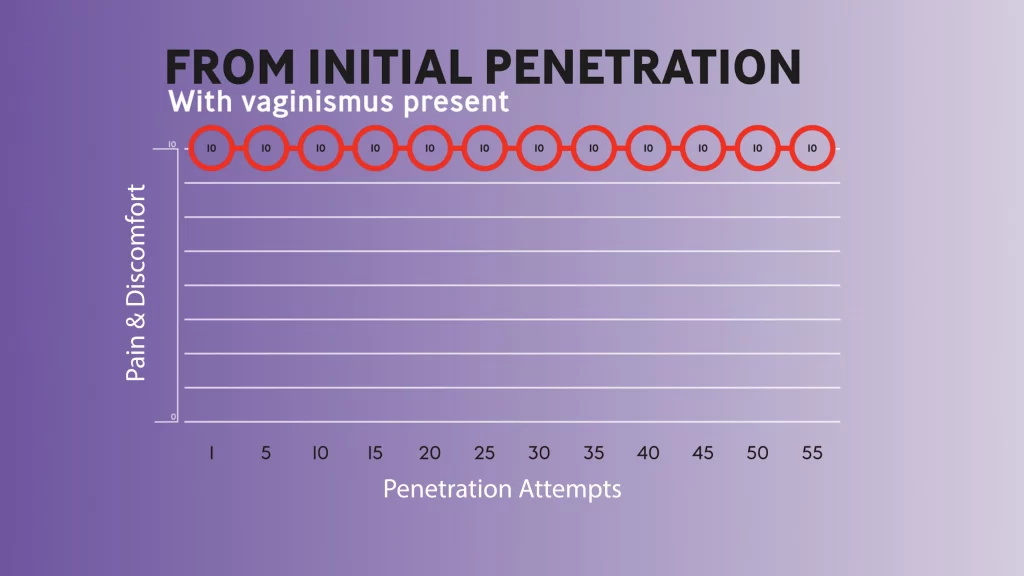
Vaginismus Response to Penetration
The second shows how, with vaginismus, there is no reduction in discomfort or pain, even with persistent practice.
Studies Into Vaginismus
As with other forms of pelvic floor dysfunction, vaginismus isn’t widely studied, however, the studies that have been completed provide some interesting insights into the condition. We have highlighted some studies in this episode. The first revealed heightened sensitivity at rest2 in the pelvic floors of women with vaginismus. If you have read our page on pelvic floor dysfunction, you will have learned that the goal of any pelvic floor training is to return the pelvic floor to an optimal resting length. It is believed3 that the heightened sensitivity experienced by women with vaginismus results in increased pelvic floor hypertonicity. This could be an indication of more fight-or-flight activity in the nervous system.
This idea is somewhat bolstered by the second study4 which scanned the brains of women with vaginismus against controls without the condition. That study founds structural changes in the part of the brain responsible for anxiety and fear in the patients with vaginismus, providing the notion that vaginismus may be a fear-related condition.
In my book, I explain how the brain cannot tell the difference between what you are thinking and something that is currently happening. Worrying and fearful thoughts have a tendency to place tension into the body, and in the case of vaginismus, this could be a major contributing factor to the condition.
Diagnosis and Treatments
Getting properly diagnosed and having your vaginismus graded is a first step in your journey towards recovery. In the lower grades, some pelvic floor relaxation, meditation and cognitive behavioural therapy can go a long way towards overcoming the condition. It can be really beneficial to undertake therapy along with your partner as this can help with trust and bonding, which in turn can help communicate a message of safety to your nervous system.
In the later grades of vaginismus, dilator therapy may be suggested as an addition to the other exercises and therapies. We’ve shared an earlier article on 5 steps to overcome vaginismus, and have created pages in our knowledge portal sharing information on the condition and it’s conservative and invasive treatments. You will find a lot of information in my book and I have just opened the discounted presale of my course on overcoming vaginismus which will be released on March 18th 2022. If you have questions, jump over to our newly launched community where you will find a space specifically for vaginismus.
References
- Pacik PT, Geletta S. Vaginismus Treatment: Clinical Trials Follow Up 241 Patients. Sex Med. 2017 Jun;5(2):e114-e123. doi: 10.1016/j.esxm.2017.02.002. Epub 2017 Mar 28. PMID: 28363809; PMCID: PMC5440634.
- Frasson E, Graziottin A, Priori A, Dall’ora E, Didonè G, Garbin EL, Vicentini S, Bertolasi L. Central nervous system abnormalities in vaginismus. Clin Neurophysiol. 2009 Jan;120(1):117-22. doi: 10.1016/j.clinph.2008.10.156. Epub 2008 Dec 13. PMID: 19071060.
- Unal, Suheyla & Soylu, Ahmet & Yılmaz, Uğur & Karlıdağ, Rifat & Özcan, Abdulcemal & BAydinc, Can. (2002). Vaginismus:Possible role of symphatetic nervous system. 10.13140/RG.2.2.16797.41443.
- Atmaca M, Baykara S, Ozer O, Korkmaz S, Akaslan U, Yildirim H. Hippocampus and amygdala volumes in patients with vaginismus. World J Psychiatry. 2016 Jun 22;6(2):221-5. doi: 10.5498/wjp.v6.i2.221. PMID: 27354964; PMCID: PMC4919261.